
Key Takeaways
You wake up one morning and your back has seized. The pain shoots down your leg. Someone — a friend, a relative, maybe even a doctor — tells you: rest...
You wake up one morning and your back has seized. The pain shoots down your leg. Someone — a friend, a relative, maybe even a doctor — tells you: rest, don’t move—you might need surgery.
So you lie still. Days pass. The pain doesn’t improve. Eventually, you’re sent for an MRI and a surgical consult.
Here’s the issue: much of the advice patients still receive for a “slipped disc” is behind current evidence. Not all of it—but enough that it delays recovery, increases anxiety, and sometimes leads to unnecessary escalation.
What a “Slipped Disc” Actually Is
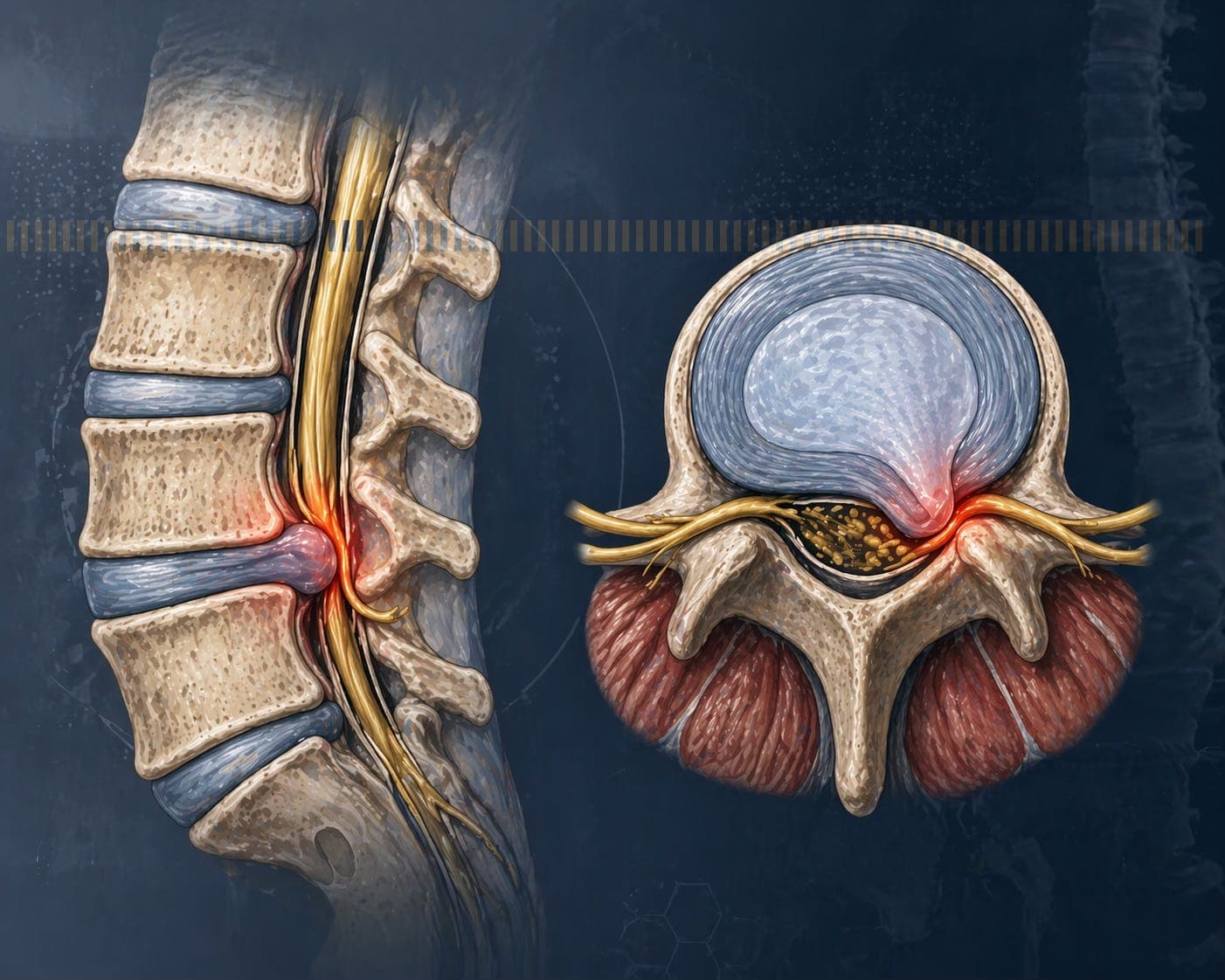
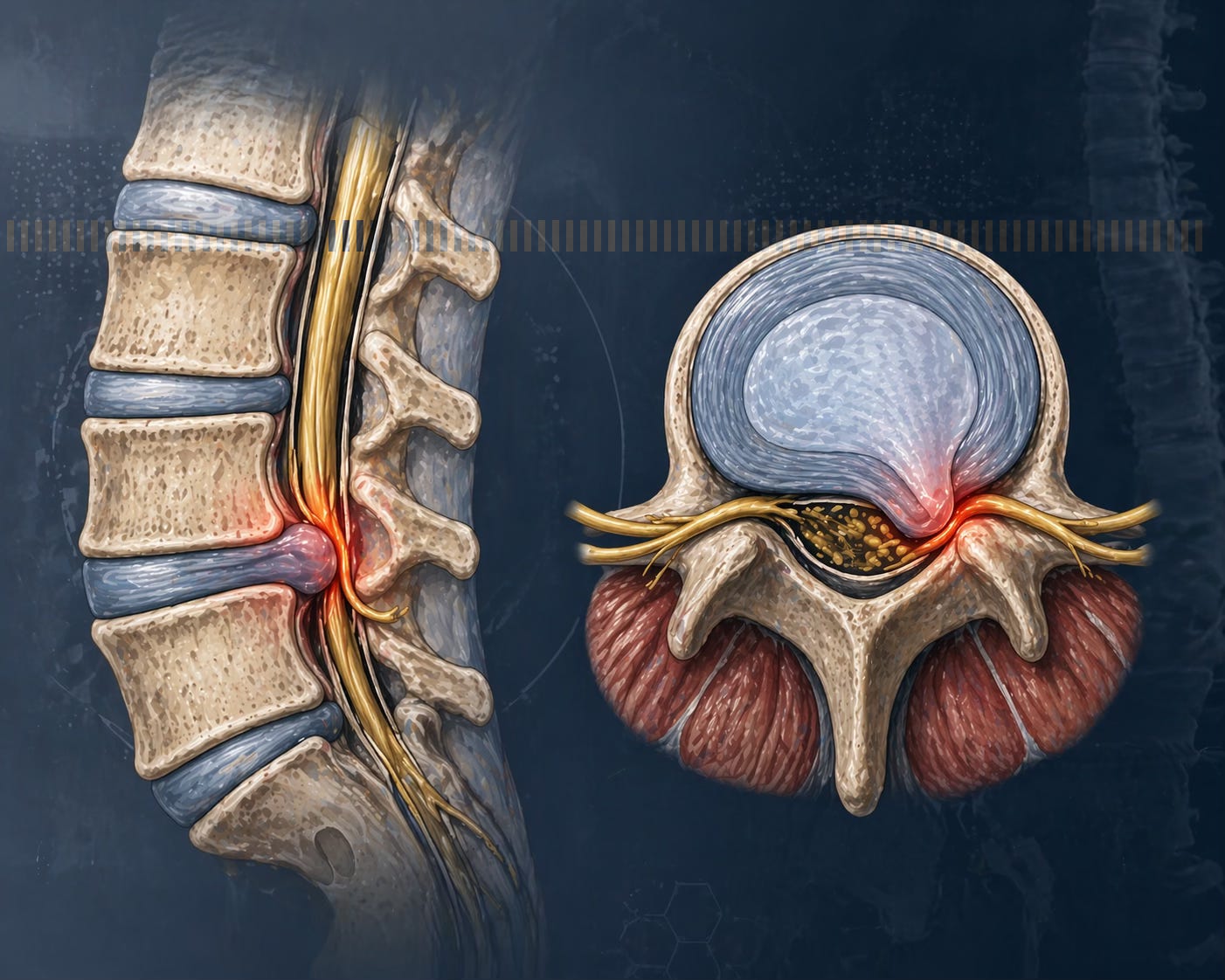
A slipped disc doesn’t actually slip. The correct term is lumbar disc herniation.
Each disc sits between your vertebrae, with a tough outer layer and a softer inner core. When the outer layer weakens, the inner material can protrude outward and irritate nearby nerves.
Pain comes from two sources:
Mechanical pressure on the nerve
Chemical irritation, driven by inflammatory molecules released by the herniated material
This is why pain can be severe even when the MRI doesn’t look dramatic. It’s also why treating it properly requires more than just rest.
Myth #1: You Should Rest
This is one of the most common—and most damaging—pieces of advice.
Modern guidelines, including those from the American Association of Neurological Surgeons, no longer recommend prolonged bed rest. A comprehensive meta-analysis of 49 studies, cited in the World Federation of Neurosurgical Societies Spine Committee consensus guidelines (2024), found that bed rest performs no better than staying active at reducing pain scores at 12 weeks.
Research consistently shows:
Bed rest performs no better than staying active
Prolonged inactivity weakens the muscles that support your spine
Movement helps discs receive nutrients and aids recovery
The current recommendation is simple:
Rest briefly during severe pain — then start moving again as early as possible.
The Part Most People Aren’t Told: Discs Can Heal on Their Own
One of the most important facts about disc herniation is also the least explained.
In many cases, the disc improves on its own.
A meta-analysis of 31 studies involving over 2,200 patients found that around 70% of herniated discs shrink or resorb over time with conservative management. The resorption process usually unfolds over 3 to 6 months, and paradoxically, the same inflammatory process that causes pain also drives the body’s repair mechanism — through macrophage infiltration and natural degradation of the herniated material (Xie et al., Orthopedic Reviews, 2023).
The real question isn’t whether recovery is possible. It’s whether you’re doing the right things to support it.
Myth #2: Surgery Is the First Answer
Surgery has a role — but for most people, it’s not the starting point.
Studies consistently show 60–80% of patients improve within weeks with conservative care, and up to 90% over time. A 2025 systematic review from Imperial College London confirmed that conservative management should be the default first-line approach, and that the benefit of surgery over conservative care largely levels off by the one-year mark.
Surgery becomes important when there are red flags:
Loss of bladder or bowel control
Rapidly worsening leg weakness or foot drop
Severe symptoms that don’t improve after adequate conservative care
For most people without these signs, the evidence supports trying structured conservative care first.
What Actually Works
The research points to a combination approach — not just one treatment.
1. Reduce the inflammatory load
A large part of disc pain comes from inflammation around the nerve root, not just mechanical pressure. Managing that inflammatory environment is a legitimate treatment target.
Conventional NSAIDs can help in the short term, though long-term use carries recognised gastrointestinal and cardiovascular risks.
A growing body of research has examined plant-derived anti-inflammatory compounds as alternatives or adjuncts. Curcuma longa (turmeric) is the most extensively studied: a 2024 randomised double-blind placebo-controlled trial found a combination of curcumin and Boswellia serrata significantly reduced pain scores and serum inflammatory markers including TNF-α and IL-6 in chronic lower back pain patients compared to placebo. Commiphora molmol (myrrh) has separately demonstrated significant analgesic and anti-inflammatory effects in peer-reviewed research. Carthamus tinctorius (safflower), long used in Chinese medicine for trauma and joint pain, has shown anti-inflammatory activity in pre-clinical studies including suppression of TNF-α and IL-1β. And Cinnamomum camphora (camphor) is one of the most widely used topical analgesics globally, with documented anti-inflammatory and analgesic activity in pharmacological research.
These compounds are not equivalent in evidence strength — curcumin and Boswellia have the strongest clinical trial data, while others are supported by pre-clinical and traditional use evidence. But collectively they represent a class of botanical anti-inflammatories with meaningful pharmacological rationale and a more favourable long-term safety profile than chronic NSAID use.
2. Move — but correctly
Exercise is one of the most effective treatments for disc herniation. A 2025 systematic review and meta-analysis found consistent improvements in pain, range of motion, and disability across eight randomised controlled trials involving 611 participants.
Exercise helps by:
Strengthening the muscles that support your spine
Improving movement and flexibility
Supporting the disc’s natural recovery process
The key is progressive, guided movement — not aggressive exercise in the acute phase, and not prolonged rest.
3. Combine movement with hands-on treatment
Physiotherapy and manual therapy help restore range of motion, reduce nerve irritation, and correct protective movement patterns. The combination consistently outperforms either approach alone.
What We See at Yapchankor
Most conservative care treats these elements separately — medication first, physiotherapy later. We do both from the start.
Our approach combines topically applied botanical anti-inflammatory compounds with structured physiotherapy, applied together from the first session.
In an internal non-controlled case review of 174 patients (November 2013), we looked at a subset of 16 patients with slipped disc conditions. Across an average of 14 sessions, we observed:
Pain reduced by 78.4% (VAS scale: from 6.38 to 1.38)
Range of motion improved by 79.2%
Muscle strength improved by 29.4%
These are observational findings from a non-controlled retrospective review — not a clinical trial. There was no control group and the sample was small. But they reflect a consistent pattern we see in practice:
When inflammation is addressed and movement is restored at the same time, recovery tends to happen faster.
The standard care timeline for chronic disc conditions is often estimated at six months or more. That is not what we commonly observe when both approaches are applied together from the outset.
Three Patterns That Slow Recovery
After decades treating back and disc conditions, we recognise recurring patterns that affect outcomes:
Pain improves, then returns. The disc improves — but the way the patient moves hasn’t reset. Unconscious guarding patterns and compensatory habits remain. Without addressing these, relapse is predictable.
Pain shifts location. Lower back pain that migrates over weeks to the hip, then the outer thigh, then the calf is typically radicular pattern migration as nerve root involvement evolves. It is frequently misread as “spreading” injury when it is not.
Pain persists despite rest. Counter-intuitively, patients who rest the most sometimes have the most persistent pain. When the dominant driver is chemical nerve irritation rather than mechanical compression, rest does not address the source.
Recognising which pattern is present helps direct treatment more precisely — rather than applying the same protocol to everyone.
The Bottom Line
A slipped disc is not a life sentence — and for most people, it is not a surgical condition.
The evidence supports early movement, structured rehabilitation, and managing the inflammatory component. The real issue is not whether conservative care works. It’s whether the care being used is active rather than passive, targeted rather than generic, and applied early enough.
Not sure what’s driving your pain? That’s often the difference between a slow recovery and a fast one. If you’ve been told to “rest and wait,” it may be worth getting a second opinion based on current evidence.
References
Al Qaraghli & De Jesus – Lumbar Disc Herniation, StatPearls (2024)
Madhivanan et al. – WFNS Spine Committee conservative treatment guidelines (2024)
Thavarajasingam et al. – Surgery vs conservative care systematic review, Brain and Spine (2025)
Zhong et al. – Spontaneous resorption meta-analysis, Pain Physician (2017)
Xie et al. – Mechanisms of resorption, Orthopedic Reviews (2023)
Du et al. – Exercise therapy meta-analysis, Frontiers in Medicine (2025)
Agarwal et al. – Curcumin + Boswellia RCT for chronic lower back pain (2024)
Shalaby & Hammouda – Commiphora molmol analgesic and anti-inflammatory activity (2015)
Wang et al. – Carthamus tinctorius anti-inflammatory activity, J Ethnopharmacology (2014)
Current Insights on Cinnamomum camphora – anti-inflammatory and analgesic review (2022)
Yapchankor Pain Treatment Centre has been treating chronic pain conditions since 1979, with clinics across Malaysia. This article is intended for general educational purposes and does not constitute medical advice. If you are experiencing back pain or neurological symptoms, please seek professional assessment for your individual condition.